As much as I complain I realize I do have many things to be thankful for, even with a chronic illness. I recently turned 28, and part of my birthday practice every year is to reflect on the most important and precious things in my life. Sometimes these things change, but some never do. I figured I should share these things with you...
I am thankful....
... that I have a loving and supportive family. We have our eccentricities, but I know they love me and I hope they know I love them. I try to show that to them as much as I can. We fight, we cry, but we're very functional.
... for my grandmother's life. She passed away between birthdays 27 and 28 and I couldn't be more grateful to have known her.
... for friends that actually care and take an interest. I have cultivated friendships with people that feel mutual and not like I'm using them or vice versa.
... for a stable, adult relationship that doesn't cause me more drama or create negative situations for me.
... that I seem to have finally wrapped my head around some parts of my illness. It's challenging and complicated, but I'm really glad I have a smart enough brain to think it out.
... that my sinuses don't get badly infected and that PO antibiotics still work well for me.
... that my insurance pays for my IVIG treatment.
... for my mobility, even if it isn't perfect all the time, it's nice to be able to walk around and go the places I want to without too much assistance.
... for unrestricted food. Many of my friends have to eat limited diets because of their disease progression and manifestations. Boy am I glad I have food freedom!
... for music.
... that there is real beauty to experience in the world.
... for last November's trip to Hawaii. I didn't know if I would ever get to go there, but I can tell you it's a magnificent experience. You should definitely do it.
... that I have people I can call if I get into trouble and need help.
This is the short list. There are more things, obviously, but these are the most important to me right now.
Wednesday, August 31, 2011
Tuesday, August 30, 2011
The Vanity Line
Where do you draw the line to say something is vanity rather than a real concern?
I ask this because I'm pretty sure the drug I've been taking to quell my autoimmune problems is making me lose my hair.
I realize that this is a small issue, but I'm supposed to be on this drug forever. It isn't like a temporary chemo-related hair loss. I'm not exactly sure how to deal. I'm going to have other things checked to eliminate all other possibilities, but I really feel in my heart of hearts that I shouldn't be taking the plaquenil anymore.
This leads to additional questions, not the least of which is "If not plaquenil, what?" because, jeez o pete, I just don't know. Maybe something will be revealed by compliment and other testing this month at the immuno so we can determine a new plan of attack.
Just when I thought things were getting better...
I ask this because I'm pretty sure the drug I've been taking to quell my autoimmune problems is making me lose my hair.
I realize that this is a small issue, but I'm supposed to be on this drug forever. It isn't like a temporary chemo-related hair loss. I'm not exactly sure how to deal. I'm going to have other things checked to eliminate all other possibilities, but I really feel in my heart of hearts that I shouldn't be taking the plaquenil anymore.
This leads to additional questions, not the least of which is "If not plaquenil, what?" because, jeez o pete, I just don't know. Maybe something will be revealed by compliment and other testing this month at the immuno so we can determine a new plan of attack.
Just when I thought things were getting better...
Diagnoses
Sometimes, I just want to scream at people...
YOUR DIAGNOSIS IS NOT WHAT YOU THINK IT IS OR WHAT YOU KEEP CALLING IT!
Yeah, so, hypogammaglobulinemia is NOT a disease. It's a symptom. Just because it has an ICD-9 code doesn't make it a diagnosis. If you have low IgG and still respond to titers, you have selective IgG deficiency. If you have low in several immunoglobulin categories (which is the definition of hypogamma) you have CVID. Furthermore, it's hypogammaglobulinemia NOT hypogammaglobulin anemia. GAH!
I know this kind of precision doesn't matter to most people, but I think it is critical that we all at least speak the same language. If your physician has diagnosed you with this, perhaps it's time to ask some questions. If you look at the IDF website that lists every recognized primary immune deficiency, you will not see hypogammaglobulinemia on the list. It's time for more questions, people, because what you're talking about is a symptom, not the disease. This leads to confusion, etc.
Most of you that read this have noooo idea what I'm talking about. Some of you do, and some of you will differ with me. I'm talking medical literature. Your doctor could, in this case, be wrong.
YOUR DIAGNOSIS IS NOT WHAT YOU THINK IT IS OR WHAT YOU KEEP CALLING IT!
Yeah, so, hypogammaglobulinemia is NOT a disease. It's a symptom. Just because it has an ICD-9 code doesn't make it a diagnosis. If you have low IgG and still respond to titers, you have selective IgG deficiency. If you have low in several immunoglobulin categories (which is the definition of hypogamma) you have CVID. Furthermore, it's hypogammaglobulinemia NOT hypogammaglobulin anemia. GAH!
I know this kind of precision doesn't matter to most people, but I think it is critical that we all at least speak the same language. If your physician has diagnosed you with this, perhaps it's time to ask some questions. If you look at the IDF website that lists every recognized primary immune deficiency, you will not see hypogammaglobulinemia on the list. It's time for more questions, people, because what you're talking about is a symptom, not the disease. This leads to confusion, etc.
Most of you that read this have noooo idea what I'm talking about. Some of you do, and some of you will differ with me. I'm talking medical literature. Your doctor could, in this case, be wrong.
Tuesday, August 23, 2011
The Cost of Noncompliance
Let's just say that sometimes, I'm an idiot. I know this about myself, it is truly not news. Sometimes, though, I am in utter awe of my stupidity and the silly things I do. My recent less-than-compliant behavior is a great example.
Apparently, I decided that being on vacation meant I didn't have to take my medication. I'll let that sink in for a minute. Lalala no pills 2x per day lalala. I got out of the habit of taking my plaquenil. I was already not great about it... Then vacation came and I lost all will to take my medicine as directed. It's really not that much to take in the grand scheme of things, but I wanted to be like the other kids, dammit. Or, more accurately, I just didn't want to have to think about it.
I have to think about it now, that's for certain. Why did I do this to myself? I know if I am noncompliant bad things happen. I start to feel more fatigued than ever... I was about to fall asleep at my desk last week... And still I didn't start being fully compliant until... YESTERDAY!?!?!? I have had bad pain and fatigue and everything else, but I was like LALALA NO PILLS! Look where that has landed me... At least it was only for a week or so, but still. I am a loser for not taking my meds like I should. I know this is a problem that many people struggle with, so I've decided to be completely honest here...
I am in pain (albeit less pain now than, say, Sunday) but every moment of it is my own darn fault.
Apparently, I decided that being on vacation meant I didn't have to take my medication. I'll let that sink in for a minute. Lalala no pills 2x per day lalala. I got out of the habit of taking my plaquenil. I was already not great about it... Then vacation came and I lost all will to take my medicine as directed. It's really not that much to take in the grand scheme of things, but I wanted to be like the other kids, dammit. Or, more accurately, I just didn't want to have to think about it.
I have to think about it now, that's for certain. Why did I do this to myself? I know if I am noncompliant bad things happen. I start to feel more fatigued than ever... I was about to fall asleep at my desk last week... And still I didn't start being fully compliant until... YESTERDAY!?!?!? I have had bad pain and fatigue and everything else, but I was like LALALA NO PILLS! Look where that has landed me... At least it was only for a week or so, but still. I am a loser for not taking my meds like I should. I know this is a problem that many people struggle with, so I've decided to be completely honest here...
I am in pain (albeit less pain now than, say, Sunday) but every moment of it is my own darn fault.
Wednesday, August 17, 2011
WMATA's Disability Application
I was thinking this morning about disabilities. If you've read many of my posts, you know I contemplate this on a pretty regular basis. This time, I was sparked by the large signage about disability fares on WMATA. I have an ADA Disability that requires accommodation, so I should qualify... should being the operative word.
I went to WMATA's website to further investigate their policies. There are some things I am beginning to feel I should take care of before I something happens, as a kind of insurance policy against the future, and this is one of those things. Especially since the disability office has the worst hours known to man. Why are they only open 8:30 AM to 4:30 PM on some days and 8:30 AM to 2:30 PM on others? Because they're WMATA.
Anyway, I found their policies on the application but I found it to be a little quizzical. I expected that my doctor would be required to fill out the form, that's fine, but the categories they have are interesting and as follows:
Ok, so most of this seems reasonable to me... until you get to #12. Autoimmune deficiencies? Do you mean Autoimmune Diseases and Immune Deficiencies? I mean, my illness is characterized by joint pain and fatigue, so I'm pretty sure my doctor will sign off, but I really wish it was more clear. I also fear that, since I don't have a listed diagnosis, approval will be challenging. I am hopeful it won't, but I don't think I have the courage or desire to start the process now. Maybe by the time my next treatment comes around, I'll be ready.
UPDATE: This little gem is also a little troubling to me... Granted, none of my things are contageous, but things like TB and HIV are...
I went to WMATA's website to further investigate their policies. There are some things I am beginning to feel I should take care of before I something happens, as a kind of insurance policy against the future, and this is one of those things. Especially since the disability office has the worst hours known to man. Why are they only open 8:30 AM to 4:30 PM on some days and 8:30 AM to 2:30 PM on others? Because they're WMATA.
Anyway, I found their policies on the application but I found it to be a little quizzical. I expected that my doctor would be required to fill out the form, that's fine, but the categories they have are interesting and as follows:
1. NON-AMBULATORY: An individual is unable to walk and requires the use of a wheelchair or other mobility device.
2. SEMI-AMBULATORY: An individual has a chronic condition, which substantially limits the ability to walk, or is unable to walk without the use of a caliper leg brace, walker or crutches.
3. AMPUTATION: An individual has an amputation of one or both hands, arms, feet, or legs.
4. STROKE: An individual has substantial functional motor deficits in any of two extremities, loss of balance and/or cognitive impairments three months post stroke.
5. NEUROLOGICAL CONDITIONS OTHER THAN STROKE: An individual has difficulty with coordination, communication, social interaction and/ or perception from a brain, spinal or peripheral nerve injury or illness, has functional motor deficits, or suffers manifestations that significantly reduce mobility. A specific diagnosis is required.
6. PULMONARY OR CARDIAC CONDITIONS: An individual has a pulmonary or cardiac condition resulting in marked limitation of physical functioning and dyspnea during activities such as climbing steps and/or walking a short distance. * If diagnosis is asthma, please state whether: a) Individual has been on systemic medication for the immediate past six months, OR b) Individual has been required to use fast acting inhaler for three or more episodes per week for the immediate past six months. A specific diagnosis is required.
7. BLIND OR LOW VISION: An individual is legally blind, whose visual acuity in the better eye, with correction, is 20/200 or less, or who has tunnel vision to 10 degrees or less from a point of fixation or so the widest diameter subtends an angle no greater than 20 degrees. An individual has low vision, and whose visual acuity is
in the range of 20/70 to 20/200 with best correction.
8. DEAF OR HARD OF HEARING: An individual with a pure tone average greater than 70 dB in both ears, regardless of use of hearing aids.
9. EPILEPSY: An individual has had at least one tonic-clonic seizure within the past
four months.
10. DEVELOPMENTAL OR LEARNING DISABILITIES: An individual has a significant learning, perceptual and/ or cognitive disability. Some conditions are excluded from eligibility such as attention deficit disorder (ADD). A specific diagnosis is required.
11. MENTAL ILLNESS: An individual whose mental illness includes a substantial disorder of thought, perception, orientation, or memory that impairs judgment and behavior. A specific diagnosis is required.
12. CHRONIC PROGRESSIVE DEBILITATING CONDITIONS: An individual who experiences debilitating diseases, autoimmune deficiencies, or progressive and uncontrollable malignancies, any of which are characterized by fatigue, weakness, pain and/or changes in mental status that impair mobility. A specific diagnosis is required.
Ok, so most of this seems reasonable to me... until you get to #12. Autoimmune deficiencies? Do you mean Autoimmune Diseases and Immune Deficiencies? I mean, my illness is characterized by joint pain and fatigue, so I'm pretty sure my doctor will sign off, but I really wish it was more clear. I also fear that, since I don't have a listed diagnosis, approval will be challenging. I am hopeful it won't, but I don't think I have the courage or desire to start the process now. Maybe by the time my next treatment comes around, I'll be ready.
UPDATE: This little gem is also a little troubling to me... Granted, none of my things are contageous, but things like TB and HIV are...
Who is not eligible: People whose sole incapacity is pregnancy, obesity, acute or chronic alcoholism or drug addiction, or have a contagious disease. Financial need is NOT a consideration.
Tuesday, August 16, 2011
Whooping Cough Vaccination
Sorry for the hiatus from posting. I took a little vacation.... but worry not! Back to business as usual.
The Virginia Department of Health is urging parents to have their children receive the Tdap vaccine for tetanus, diphtheria and pertussis (aka whooping cough) in no small part because there has been a 217% increase in whooping cough cases in Virginia in the first 6 months of this year. (article
here) Whooping cough is scary, especially since it is so communicable. So next time you're due for your tetanus vaccine, ask specifically for tdap. It could save your life or the life of someone you love.
Read a little more about pertussis and get vaccinated!
The Virginia Department of Health is urging parents to have their children receive the Tdap vaccine for tetanus, diphtheria and pertussis (aka whooping cough) in no small part because there has been a 217% increase in whooping cough cases in Virginia in the first 6 months of this year. (article
here) Whooping cough is scary, especially since it is so communicable. So next time you're due for your tetanus vaccine, ask specifically for tdap. It could save your life or the life of someone you love.
Read a little more about pertussis and get vaccinated!
Tuesday, August 9, 2011
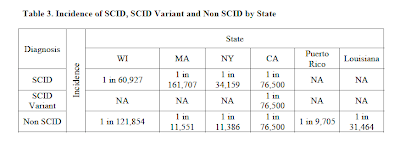
SCID Newborn Screening: One Year Later
The Health Resources and Services Administration has released the report it submitted to the Secretary of Health and Human Services Kathleen Sebelius one year after adding SCID screening Recommended Uniform Screening Panel. Some of the highlights:
*To date, 961,925 newborns have been screened and 60 infants, or approximately 1 in 16,032, have been identified with some form of immune deficiency.
*Fourteen infants with SCID (~1 in 68,000) have been diagnosed and received treatment.
*No missed cases of SCID have come to the attention of the newborn screening programs conducting the pilots.
*Emerging findings from the pilots are advancing understanding of SCID and triggering new research efforts.
(All items taken from the report which can be downloaded in PDF format here.)
This is amazing! I am a little stunned by the numbers they mention in the report. I know I had heard about increased incidence among hispanic and closed populations, but I was really surprised by the Puerto Rico findings. I'm hopeful that perhaps this report can help encourage other states to go forward with screening efforts. Let's increase this from covering 25% of US births to 100%!
*To date, 961,925 newborns have been screened and 60 infants, or approximately 1 in 16,032, have been identified with some form of immune deficiency.
*Fourteen infants with SCID (~1 in 68,000) have been diagnosed and received treatment.
*No missed cases of SCID have come to the attention of the newborn screening programs conducting the pilots.
*Emerging findings from the pilots are advancing understanding of SCID and triggering new research efforts.

(All items taken from the report which can be downloaded in PDF format here.)
This is amazing! I am a little stunned by the numbers they mention in the report. I know I had heard about increased incidence among hispanic and closed populations, but I was really surprised by the Puerto Rico findings. I'm hopeful that perhaps this report can help encourage other states to go forward with screening efforts. Let's increase this from covering 25% of US births to 100%!
Monday, August 8, 2011
Doctor Patient Relationships
My medical team is awesome. We've discussed this before. I'm starting to form my own methods and opinions for how I've developed rapport with doctors. It's something that has taken a significant investment on my part, and some willingness to listen on theirs.
I think the difference for me has been becoming insistent. I had some of the same symptoms for a long time before I started trying to address them with my doctors. Sometimes, they were dismissive or wanted me to wait. It was when I decided to take more ownership and drive my own care that things began to change for me and I began to feel better about my level of care.
I didn't change doctors to accomplish this. I started doing research and asking better questions. I started connecting my symptoms and being more willing to discuss them in detail, making notes to ensure I didn't leave things out. I really wanted to understand what was going on with my care and wanted my doctors to understand how these things were making me feel physically. It has gotten to the point where my doctors now even ask about my emotional health. This is a major change for me.
I won't pretend that any of this was easy. It has taken years to get to this point, but now I go in to my appointments with more confidence. I discuss with my doctors the treatment plan, look at various options, and make sure we're all on the same page. It feels wonderful to be able to do that. My caveat would be that you must approach them in a professional, collegial manner. That's been the big key for me. I have utmost respect for my physicians, but I no longer fear them or just sit quietly while they dictate the treatment plan. Not every doctor will engage like this, but I think a lot more of them will than you might first think.
I know a lot of people struggle with this balance of asking questions but not seeming to be too aggressive. It takes time to learn and I think it's important to try. Small steps at first, like discussing all the available medications for a specific symptom, or even figuring out what OTC cold medications are right for you. These little things can begin to change the way you see your doctors and vice versa. You may also learn that things you've "always done" aren't necessarily the best or most advantageous for your body. Don't be afraid. Odds are your doctor wants you to be as healthy as possible, just like you do.
I think the difference for me has been becoming insistent. I had some of the same symptoms for a long time before I started trying to address them with my doctors. Sometimes, they were dismissive or wanted me to wait. It was when I decided to take more ownership and drive my own care that things began to change for me and I began to feel better about my level of care.
I didn't change doctors to accomplish this. I started doing research and asking better questions. I started connecting my symptoms and being more willing to discuss them in detail, making notes to ensure I didn't leave things out. I really wanted to understand what was going on with my care and wanted my doctors to understand how these things were making me feel physically. It has gotten to the point where my doctors now even ask about my emotional health. This is a major change for me.
I won't pretend that any of this was easy. It has taken years to get to this point, but now I go in to my appointments with more confidence. I discuss with my doctors the treatment plan, look at various options, and make sure we're all on the same page. It feels wonderful to be able to do that. My caveat would be that you must approach them in a professional, collegial manner. That's been the big key for me. I have utmost respect for my physicians, but I no longer fear them or just sit quietly while they dictate the treatment plan. Not every doctor will engage like this, but I think a lot more of them will than you might first think.
I know a lot of people struggle with this balance of asking questions but not seeming to be too aggressive. It takes time to learn and I think it's important to try. Small steps at first, like discussing all the available medications for a specific symptom, or even figuring out what OTC cold medications are right for you. These little things can begin to change the way you see your doctors and vice versa. You may also learn that things you've "always done" aren't necessarily the best or most advantageous for your body. Don't be afraid. Odds are your doctor wants you to be as healthy as possible, just like you do.
Thursday, August 4, 2011
No, Your Immune System is NOT Horrible
My poor facebook friends become blog fodder sometimes. Sorry in advance, guys.
It kind of annoys me when people rant about their "horrible" immune systems. I know I should be used to such things, but it's still annoying to hear a healthy person say they have a "horrible" immune system. Now I understand that people use this as a hyperbolic statement when discussing why they get sick, but it strikes me as strange. I'm pretty sure I get sick more often than most people, but I still wouldn't say I have a "horrible" immune system, at least not most of the time. It's just not there.
Most immune competent people don't realize how insensitive it sounds when they talk to someone who is so fundamentally broken in this important way. It's like "yeah, my immune system is bad, too." You may think you've got a bad immune system, but I'd give anything I could to have the chance to have what you do, but that will never be possible for me. No one has perfect health, and if you're exposed to new bugs, you've got a decent chance of getting sick. The difference is, you'll be well in a few days with the right care. Even with the right care, a stray bug could kill me.
I guess it's all about perspective.
It kind of annoys me when people rant about their "horrible" immune systems. I know I should be used to such things, but it's still annoying to hear a healthy person say they have a "horrible" immune system. Now I understand that people use this as a hyperbolic statement when discussing why they get sick, but it strikes me as strange. I'm pretty sure I get sick more often than most people, but I still wouldn't say I have a "horrible" immune system, at least not most of the time. It's just not there.
Most immune competent people don't realize how insensitive it sounds when they talk to someone who is so fundamentally broken in this important way. It's like "yeah, my immune system is bad, too." You may think you've got a bad immune system, but I'd give anything I could to have the chance to have what you do, but that will never be possible for me. No one has perfect health, and if you're exposed to new bugs, you've got a decent chance of getting sick. The difference is, you'll be well in a few days with the right care. Even with the right care, a stray bug could kill me.
I guess it's all about perspective.
Monday, August 1, 2011
Breast Cancer "Awareness"
As I am wont to do, I got in a discussion on Facebook about these silly, cryptic status messages. I am of the opinion that telling your shoe size in inches with a frowny face doesn't actually do anything to promote awareness or show support for breast cancer patients. In fact, I think the whole thing cheapens the experience of cancer.
Cancer sucks, I'm sure. I've never had it, but I have been very sick and have a chronic illness, so I can pretty well imagine that it would suck pretty hard. I've seen people go through chemo and it seems rough. It's not glamorous, it's not easy. I think it would be much better if people took the time to go to a chemo ward and sit with these women going through the worst experience of their lives. Hold their hands, bring them a sandwich. Actually do something meaningful.
It was pointed out to me that some people hide their cancer. I think this is well within their rights. I hid my PIDD for a long time and was reluctant to talk about the serious nature of my illness. I get that people don't want to make people feel sorry for them. That all makes sense to me, especially after having to have a needle biopsy for a lump. I verbally threatened everyone who knew that if I had cancer, they were to never ever lay hands or give to me anything with a pink ribbon. The pink ribbon movement was borne out of a sister's grief, but has taken things to a ridiculous and disrespectful level. You can now get "breast cancer awareness" themed grocery items, kitchen wares, NFL hats, and yes, even fast food. But what does buying these things do for the actual patients? They keep trying to find a cure for cancer.
You know what? I'm going to be really bold here. There is no cure for cancer. There. I said it. Cancer is the overgrowth of your body's own cells. That's what makes it so challenging to treat in the first place. It isn't some sort of virus we just need to figure out. The only way to "cure" it entirely would be to either teach the body to fight these types of cells or to stop cell growth. When your cells stop growing, you die. So I would rather we have a conversation about better, more effective, less invasive treatments for cancer, instead of this constant drumbeat about awareness and a "cure."
Cancer sucks, I'm sure. I've never had it, but I have been very sick and have a chronic illness, so I can pretty well imagine that it would suck pretty hard. I've seen people go through chemo and it seems rough. It's not glamorous, it's not easy. I think it would be much better if people took the time to go to a chemo ward and sit with these women going through the worst experience of their lives. Hold their hands, bring them a sandwich. Actually do something meaningful.
It was pointed out to me that some people hide their cancer. I think this is well within their rights. I hid my PIDD for a long time and was reluctant to talk about the serious nature of my illness. I get that people don't want to make people feel sorry for them. That all makes sense to me, especially after having to have a needle biopsy for a lump. I verbally threatened everyone who knew that if I had cancer, they were to never ever lay hands or give to me anything with a pink ribbon. The pink ribbon movement was borne out of a sister's grief, but has taken things to a ridiculous and disrespectful level. You can now get "breast cancer awareness" themed grocery items, kitchen wares, NFL hats, and yes, even fast food. But what does buying these things do for the actual patients? They keep trying to find a cure for cancer.
You know what? I'm going to be really bold here. There is no cure for cancer. There. I said it. Cancer is the overgrowth of your body's own cells. That's what makes it so challenging to treat in the first place. It isn't some sort of virus we just need to figure out. The only way to "cure" it entirely would be to either teach the body to fight these types of cells or to stop cell growth. When your cells stop growing, you die. So I would rather we have a conversation about better, more effective, less invasive treatments for cancer, instead of this constant drumbeat about awareness and a "cure."
Subscribe to:
Posts (Atom)